Introduction
Central venous catheters (CVCs) are used to administer massive fluid, blood products, and multiple parenteral medications (e.g., vasoconstrictors or sedatives) in the emergent setting. CVC placement requires proper training and is not without adverse events even when performed by skilled operators. The mechanical complications of CVCs mostly arise during punctures. However, delayed complications associated with maintenance or removal of the catheter also occur [1].
Case presentation
Case 1
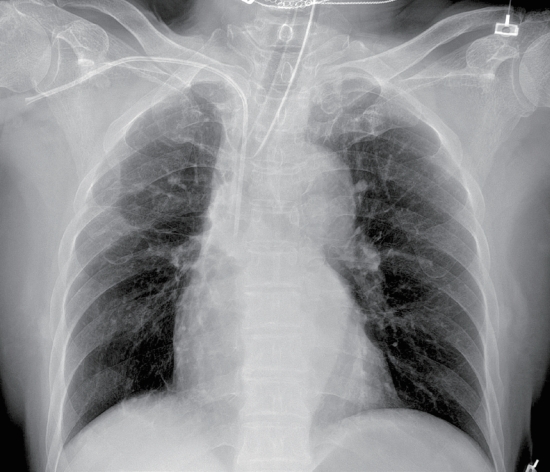
A 68-year-old female patient presented with multiple deep lacerations in both of the wrists, abdomen, and scalp from suicidal attempts. Upon arrival, the patient was unstable with a blood pressure of 70/30 mmHg and a heart rate of 133 beats per min with a Glasgow Coma Scale (GCS) score of 6. A 7-Fr CVC was inserted via the right subclavian approach for a resuscitation purpose. A post-procedural chest radiograph showed proper catheter tip placement (Fig. 1). However, unintended CVC placement in the subclavian artery (SCA) was identified later using chest computed tomography (CT) scans (Fig. 2). The distance from the skin surface to the arteriotomy was 3.8 cm. A decision was made to use a vascular closure device (VCD; FemosealTM, Terumo, NJ, USA) because the SCA could not be manually compressed. The SCA was successfully closed by endovascular VCD deployment (Video 1). A follow-up CT demonstrated the intact SCA without bleeding (Fig. 3).
Case 2
A 16-year-old male patient with a grade II traumatic spleen laceration was admitted to the intensive care unit. A 7-Fr CVC was placed in the right subclavian vein to aid in resuscitation which was removed 4 days later. The removal was performed while the patient was sitting. After a few seconds, the patient showed blurred vision, seizure, and altered mental status with a decreased GCS of 11. A brain CT was immediately performed and a cerebral air embolism (CAE) was strongly suspected (Fig. 4A). The patient was placed in the Trendelenburg position to prevent further air travel and underwent hyperbaric oxygen therapy (HBOT), which provided 100% oxygen at 2 kg/cm2. The patient made a complete neurological recovery after three cycles (50, 50, and 40 min; total=140 min) of HBOT (Fig. 4B).
Discussion
An accidental arterial puncture occurs in 2.7% of the subclavian approaches [2]; it can be unrecognized in patients with hypotension with reduced pulsatile flow. Prompt recognition and intervention are essential as prolonged arterial cannulation can result in bleeding, thrombosis, stroke, limb ischemia, neurologic deficit, or even mortality. Treatment options include open surgical repair and endovascular procedures (e.g., embolization, stent insertion, balloon inflation, or use of VCDs) [3,4].
The VCD seals the site of the arteriotomy mechanically by sandwiching two bioabsorbable discs [3]. Although the off-label use of VCDs to repair vessels other than a femoral artery lacks data, their use is still increasing [2-4]. According to a meta-analysis, the overall repair success rate of the iatrogenic thoracocervical arterial injuries via VCDs was 95.7% [4]. The current case demonstrates that the VCD is a safe and effective option for accidental CVC cannulation in the SCA. However, the treatment strategies should be tailored on a case-by-case basis, which considers the patient’s hemodynamic status, puncture site, underlying arterial conditions, and a caliber of the CVCs.
The incidence of an air embolism while insertion, manipulation, and removal of the CVCs is 0.03%-2% [5]. The CAE is a preventable complication if precautionary measures are followed during CVC removal—the head-down position, the Valsalva maneuver, and an airtight dressing [6]. Relevant imaging is needed when acute neurological symptoms occur after such procedures for early diagnosis and treatment. The HBOT, according to the United States Navy Table 6 (Fig. 5), is currently considered the standard regimen for CAE treatment [5,6]. While mortality of CAE reaches up to 20%, 75% of the survivors are reported to have mild to no disabilities with prompt HBOT treatment [6].
This report is believed to offer important lessons to all professionals who come across CVCs in daily clinical scenes. Knowing how to prevent, recognize, and manage rare complications concerned with the CVCs would decrease the chances of causing harm to patients who are already in their extremis due to polytraumas.