Introduction
Traumatic pneumocephalus is caused by air collection in the intracranial cavity after trauma. When intracranial air causes intracranial hypertension, it leads to tension pneumocephalus, which results in mass effect with neurological deterioration [1-3]. Pneumocephalus is generally diagnosed on brain computed tomography (CT) but is rarely identified on skull X-ray, as observed in this case [4].
Case presentation
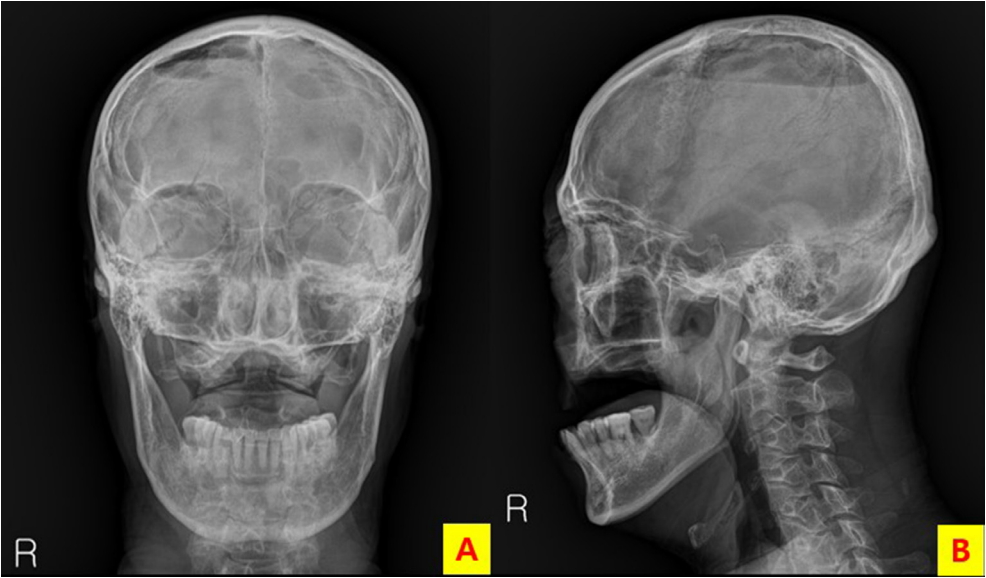
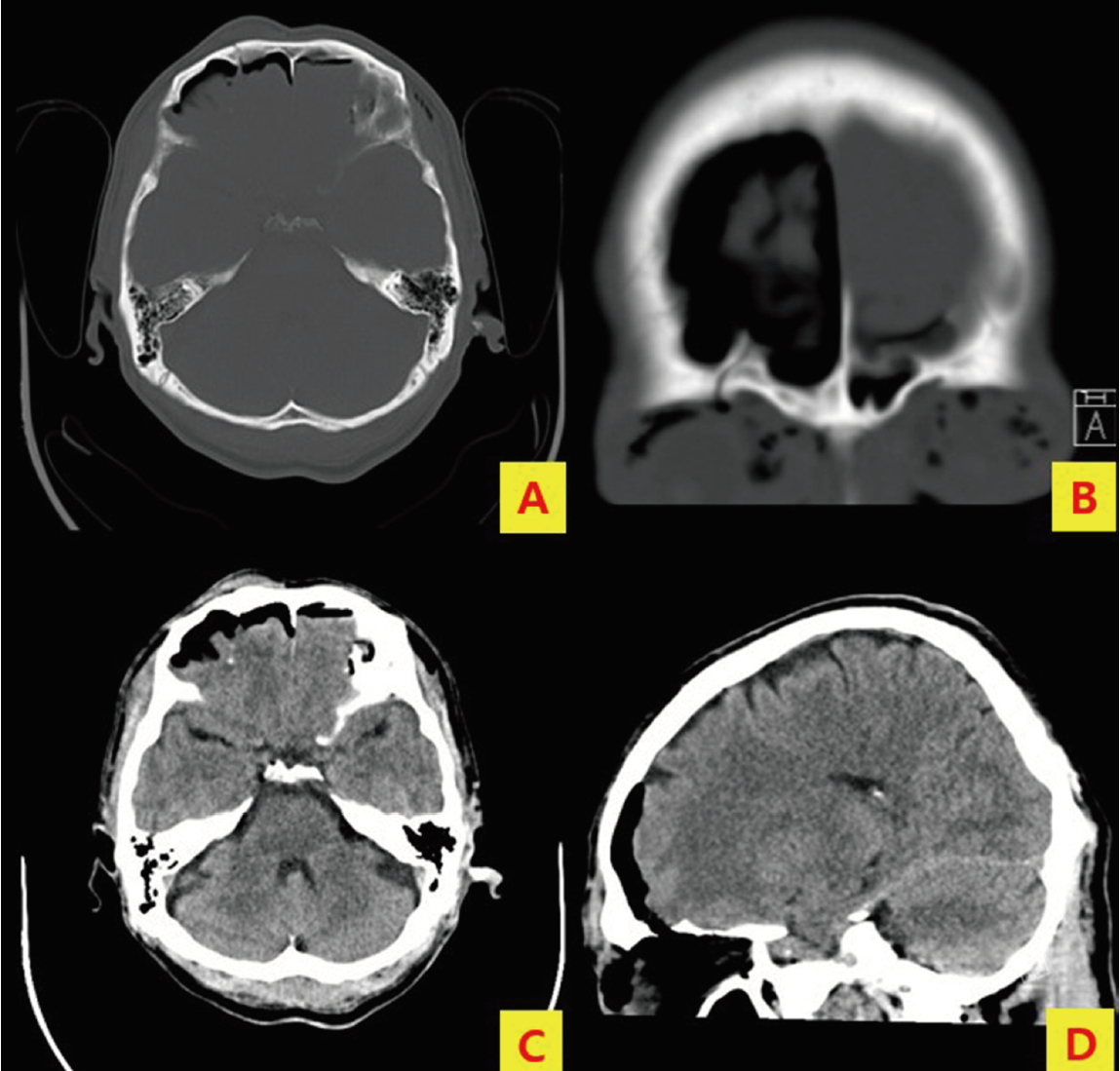
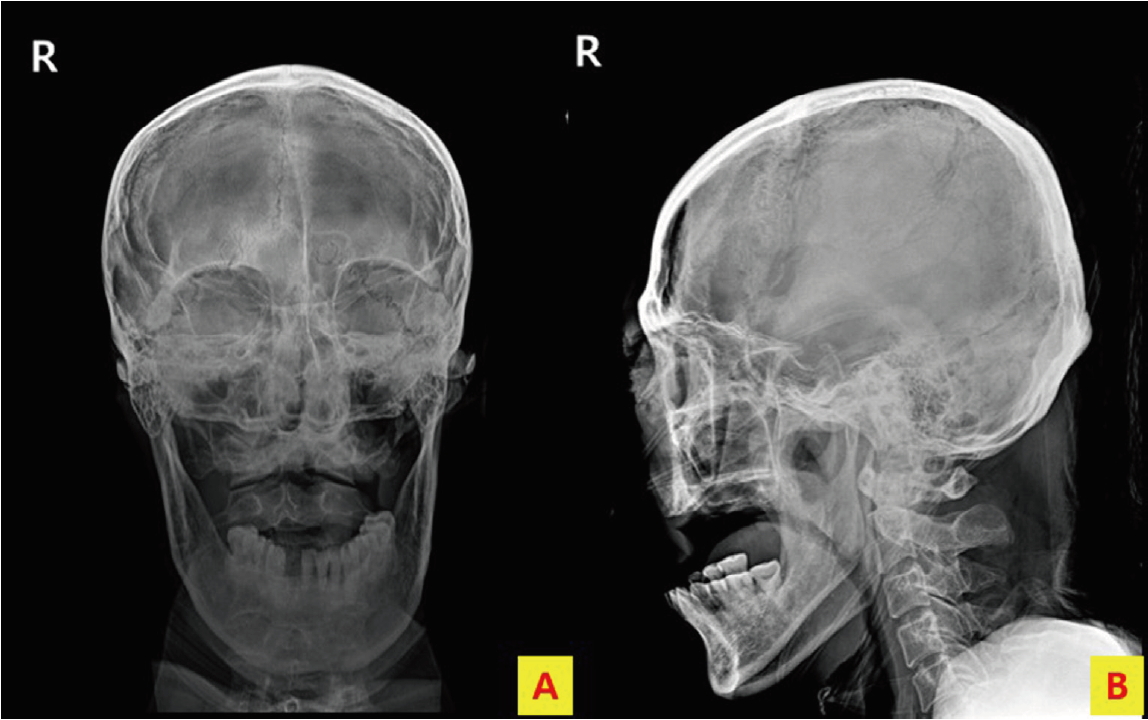
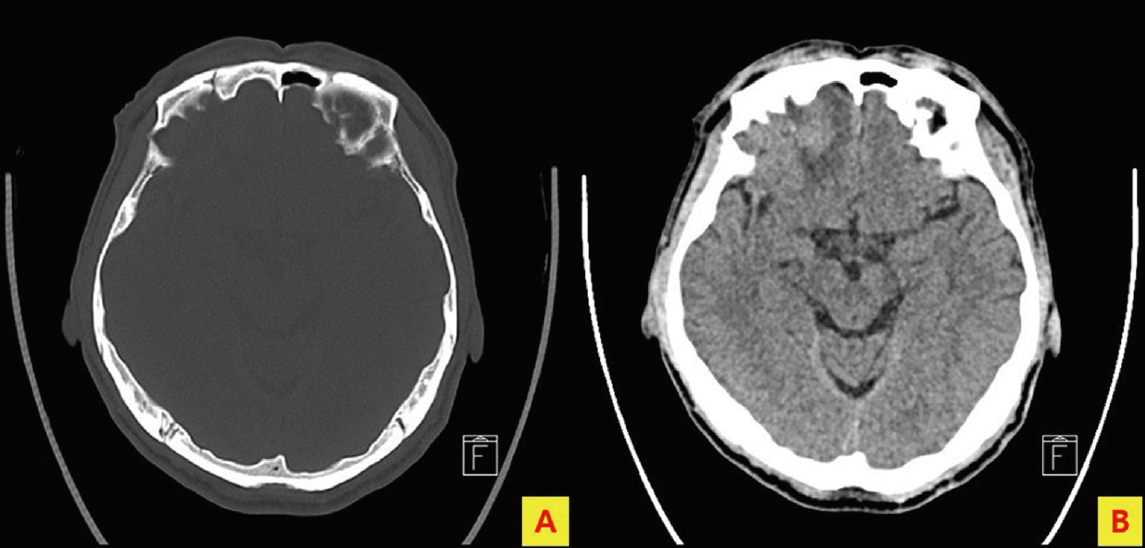
A 59-year-old man was referred to our emergency department from another hospital after falling forward from a ladder, on which he was working, at a height of 1.5 m. He complained of facial pain, had facial swelling, and his Glasgow Coma Scale was 15. Initial vital signs were as follows: blood pressure of 176/88 mmHg, pulse rate of 87 beats/min, respiration rate of 16 breaths/min, body temperature of 37.4°C, and oxygen saturation of 94%. Skull X-ray (anteroposterior [AP] and lateral views) performed in erect position at the previous hospital showed intracranial air in the parietal region (Fig. 1), and fracture of the frontal bone and pneumocephalus were observed on brain CT (Fig. 2). Skull X-ray (AP and lateral views) in supine position and brain CT performed at our hospital showed intracranial air in the frontal region (Fig. 3). Conservative treatment was adjusted, and brain CT performed on the 10th day of admission showed that the intracranial air had nearly disappeared (Fig. 4). The patient was discharged on the 14th day of admission without any complications .
Discussion
Traumatic pneumocephalus rarely progresses to tension pneumocephalus, which is accompanied by neurological deterioration and should be considered a neurosurgical emergency [1-3]. Pneumocephalus is primarily diagnosed on brain CT and is rarely observed on skull X-ray [4]. In this case, skull X-ray was performed in the erect position at another hospital, which showed presence of intracranial air in the parietal region. In contrast, at our hospital, skull X-ray was performed in the supine position, which showed presence of intracranial air in the frontal region. Observing intracranial air migration caused by position change in skull X-rays is extremely difficult because skull X-ray in erect position is rarely performed in case of patients with head injury. To the best of our knowledge, no such case has been reported in English literature. In our case, there was no neurological deterioration, conservative treatment was administered, and subsequent brain CT revealed gradual disappearance of the intracranial air.