Isolated gallbladder injury following blunt abdominal trauma: a case report
Article information
Abstract
Isolated gallbladder injury following blunt abdominal trauma is very rare. Early diagnosis of such injuries is often difficult due to their rarity and nonspecific symptoms. A surgeon’s suspicion and knowledge about the characteristic imaging findings of gallbladder injury are important. This study presents a case of gallbladder injury following blunt abdominal trauma that was diagnosed by computed tomography.
Introduction
The gallbladder is located within the gallbladder fossa on the visceral surface of the right lobe of the liver and is sheltered by the right costal margin. Its anatomical location possibly accounts for the low incidence of gallbladder injuries following blunt abdominal trauma [1]. The diagnosis of blunt injury to the gallbladder may often be difficult and delayed because of the nonspecific clinical symptoms. For early diagnosis, it is important to suspect gallbladder injury and understand the characteristic imaging findings. Here we present a case of gallbladder injury following blunt abdominal trauma that was diagnosed by computed tomography (CT).
Case presentation
A 45-year-old woman with a history of major depressive disorder was admitted to the emergency department after a fall from a height of 7 floors. She was alert and hemodynamically stable on arrival, and quadriparesis was observed. Physical examination of the abdomen did not yield reliable findings because of a cervical spinal cord injury. A whole-body scan was performed according to the trauma protocol, and C5-C6 dislocation, sternal fracture, multiple rib fractures with pneumothorax, and edematous gallbladder were revealed. The Injury Severity Score was 36. Abdominal contrast-enhanced CT showed an enlarged, edematous gallbladder, with active extravasation of intraluminal contrast medium and discontinuity of the mucosal layer (Fig. 1A, 1B). Scanty pericholecystic and perihepatic fluid was present.

Abdominal computed tomography revealed edema of the gallbladder wall, intraluminal extravasation of contrast medium (thin arrow), and discontinuity of the mucosal layer (thick arrow).
Exploratory laparoscopy confirmed that the gallbladder was enlarged and edematous and had bile-stained contents (Fig. 2A). In addition, the taeniae coli outside the transverse colon were torn (Fig. 2B), and the mucosal and muscular layers were disrupted (Fig. 2C). Cholecystectomy and suture repair of the torn taeniae coli were successfully performed with laparoscopy. The patient’s postoperative course was unremarkable .
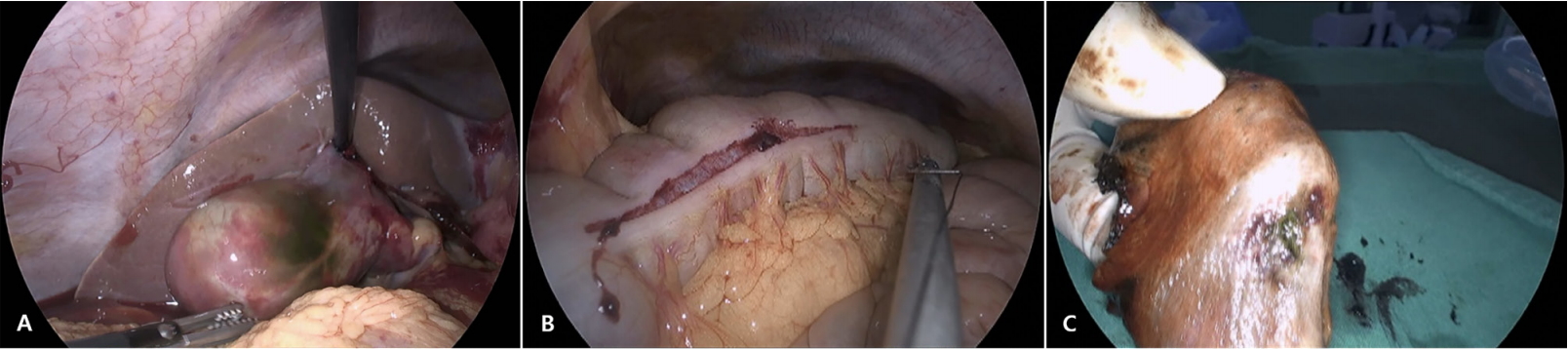
Laparoscopic findings: (A) Edematous, bile-stained, and enlarged gallbladder; (B) Torn taeniae coli on the transverse colon; (C) Disrupted mucosal and muscular layers in gallbaldder.
Discussion
Gallbladder injury is rare and found in only approximately 2% of patients who undergo laparotomy for abdominal trauma [2]. In the majority (89%) of patients, gallbladder injury is caused by penetrating trauma, whereas gallbladder injury due to blunt abdominal trauma is rare [3]. Blunt trauma is frequently associated with adjacent liver injury. Isolated gallbladder injury is very rare. Such an injury caused by blunt trauma is usually secondary to a direct blow or to shearing forces, which are more likely to cause an avulsion type of injury [2].
Isolated traumatic gallbladder injury is infrequent because of its anatomic location, given that the organ is protected by the adjacent liver and ribcage [1]. Diagnosis of isolated gallbladder injury, especially contusion to the gallbladder, is often delayed because of the lack of acute signs or symptoms, and such a delay can potentially increase the risk of morbidity [1,2]. Therefore, surgeons must consider gallbladder injury based on abnormal imaging findings.
CT is the most sensitive method for diagnosing gallbladder injury [4]. The appearance of hyperdense blood within the gallbladder lumen is highly suggestive of gallbladder injury, and an irregularity of the gallbladder wall may be the only indication of an underlying gallbladder injury [4]. The findings in our case were active hemorrhage within the gallbladder lumen and edematous wall thickening with discontinuity of the mucosal layer.
The management of gallbladder injury is based on clinical symptoms. Mild contusions may be treated conservatively. With perforation or avulsion, cholecystectomy is often the treatment of choice, and it yields favorable results [1,2]. The mortality rate of patients with gallbladder injury is related to the associated injuries. The prognosis of patients with gallbladder injury in cases of early detection and lack of other severe associated injuries remains quite good [2,5].
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.