CASE
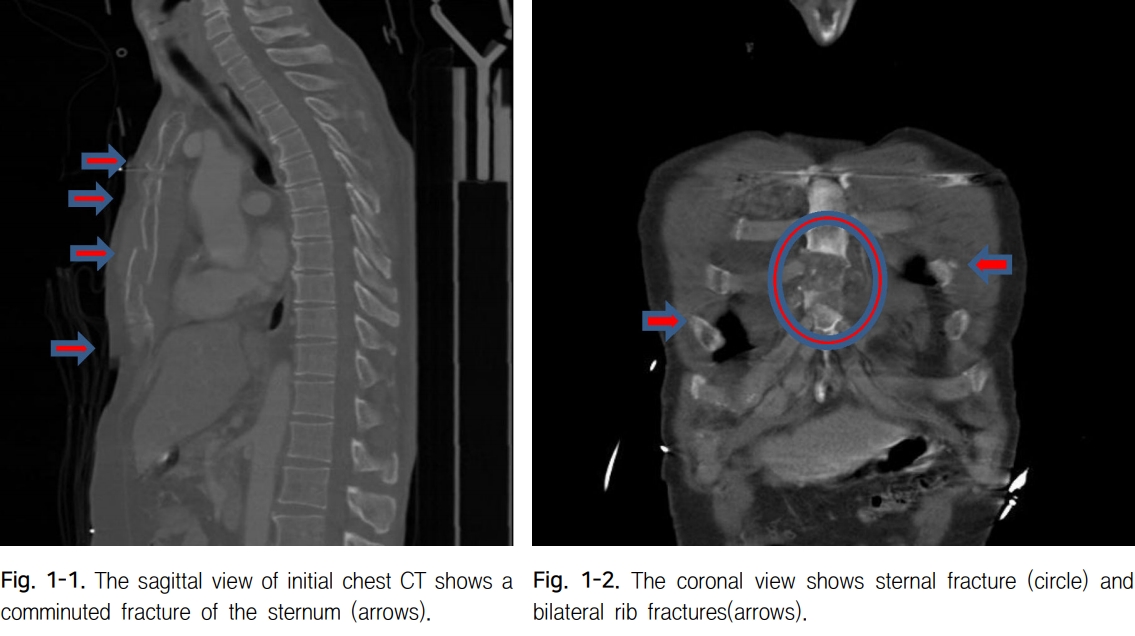
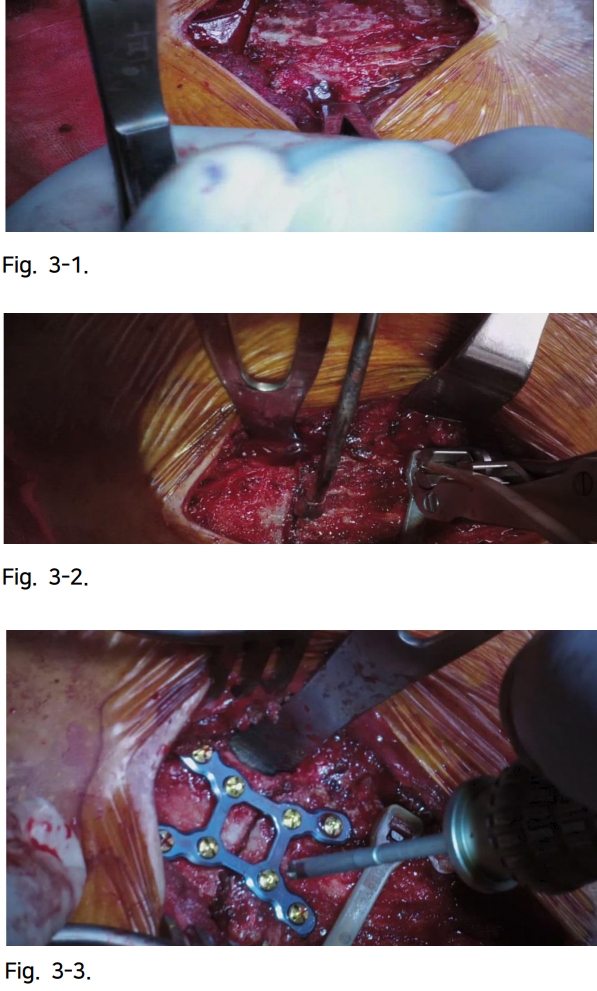
A 57-year-old male injured in a pedestrian traffic accident was transferred to our Regional Trauma Center. Immediate intubation was performed due to stupor mentality and respiratory distress at presentation. After resuscitation and physical examination, he was transferred to Trauma Intensive Care Unit. The chest computed tomography (CT) revealed multiple rib fractures at the bilateral anterior arch from 3rd to 6th ribs and comminuted fracture of the sternum (Fig. 1). He was diagnosed with anterior flail chest with concomitant injuries, i.e., fracture of the pedicle right at the 4th cervical spine, complex pelvic fracture including the right iliac wing, superior and inferior ramus of the bilateral pubis, sacrum ala, and intertrochanteric part of the right femur. On day 4 of hospitalization, rib CT was performed to evaluate sternum and rib fractures (Fig. 2). Five days later, surgical treatment was decided for the sternal fracture because weaning was still difficult despite reduced ventilator support and clear recovery of mental status. After a midline longitudinal incision between the 3rd and 5th costal notch, meticulous dissection was performed to expose healthy bones and 4th intercostal space. The DeBakey peripheral vascular clamp was used to carefully pass below the posterior segment, and then the Penrose tube was pulled and placed bilaterally (Fig. 3-1). ZipfixTM (Synthes GmbH, Oberdorf, Switzerland) was placed after the cutting needle passed through the Penrose tube. Hematoma removal was sequentially performed between the fragment and approximation, and then the ZipfixTM was tightened (Fig. 3-2). The 8-hole X plate of the SternaLockTM Blu (Biomet Microfixation Inc., Jacksonville, FL, USA) was used to transverse the fracture site (Fig.3-3). On postoperative day 2, the patient was successfully weaned from mechanical ventilation. Postoperative follow-up rib CT revealed complete approximation of the sternum (Fig. 4). No complaints associated with instability and wound problems were reported at the 3-month follow-up.
DISCUSSION
Traumatic sternal fractures have been known to occur in approximately 3%ŌĆō8% of all patients with blunt trauma. Most of these fractures are conservatively treated, and surgical fixation management in selected cases is reportedly more effective and results in good progress [1].
In this case, the patient was diagnosed with anterior flail chest with concomitant multiple injuries involving the spine, extremities, pelvis, and bladder; thus, requiring multiple surgeries and long-term immobilization through bed rest. Moreover, despite conservative ventilation management, patients with anterior flail chest are expected to require longer mechanical ventilation.
There is no definitive optimal surgical fixation time of the sternum with anterior flail chest. However, management of anterior flail chest has been reported with only pneumatic stabilization that needed mechanical ventilation for 15.6 days, and among them, the patient with displaced sternal fracture required sternal fixation [5]. In our case, the patient needed sufficient time to confirm full mental status recovery and sternum and rib fracture evaluation because the initial chest CT showed unclear findings due to the presence of artifacts.
Several surgical techniques and options existed for anterior flail chest [2, 3]. In our case, the SternaLockTM plating and ZipFixTM systems were used because the posterior lower fragment of the fracture was separated from the anterior and remained only in thin layer; therefore, incomplete approximation and iatrogenic fracture were suspected.
The ZipFixTM system is a cable-tie-based sternal closure system used to close the sternum after a median sternotomy during cardiac surgery. It is relatively flexible and provides low profile height over the sternal bone [4]. As in our case, it was considered to provide good reduction and approximation without risks of iatrogenic fracture for the thinner fragment in the coronal separated sternal fracture.
This technique is considered to be a feasible method to surgically fix this type of sternal fracture in anterior flail chest.