CASE
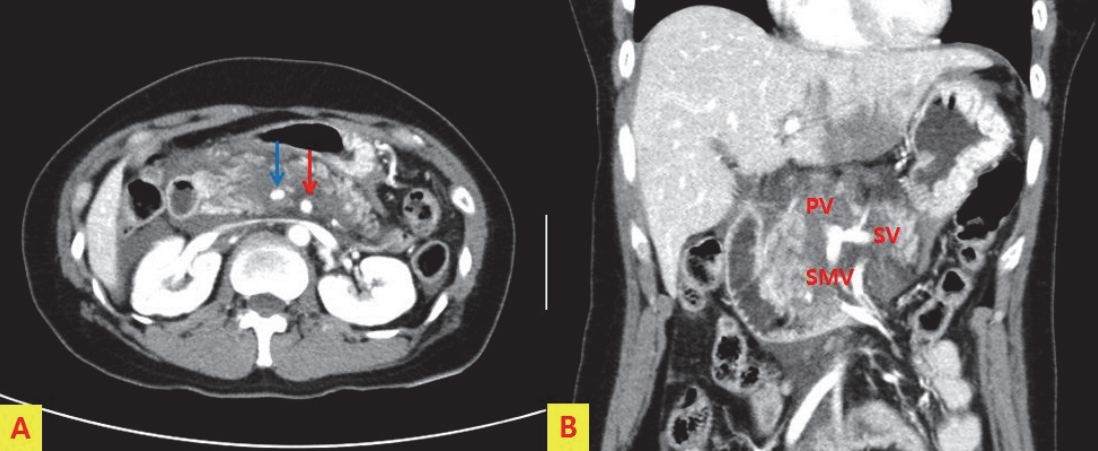
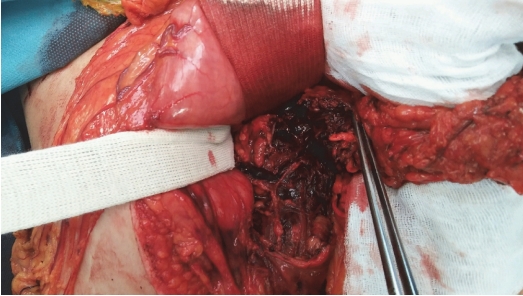
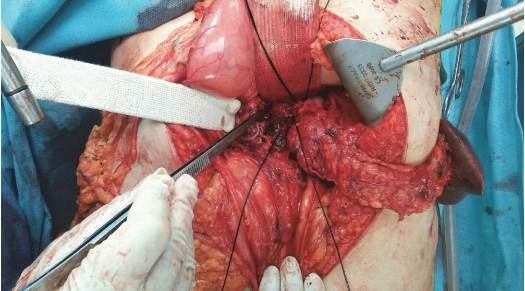
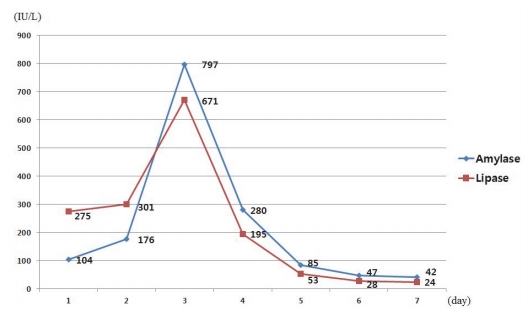
A 43-year-old woman who had been in a traffic accident was referred to our emergency department from another hospital after a driver traffic accident. Her initial vital signs were unstable: blood pressure, 75/58 mm Hg; pulse rate, 95 beats/min; respiration rate, 18 breaths/min; body temperature, 36.8°C; and oxygen saturation, 98%. Abdominal computed tomography (CT) performed at another hospital revealed complete transection of the pancreas to the right of the superior mesenteric vein (Fig. 1.). Injury severity score of the patient was 57. Emergency surgery was performed, and pancreatic transection was observed (Fig. 2.). The splenic artery and vein were ligated at their proximal portions (Fig. 3.), and subtotal pancreatectomy was performed (Fig. 4.). After ligation of the main pancreatic duct in the remnant pancreas, the pancreatic stump was closed by fish-mouth interrupted sutures. The initial serum amylase and lipase levels were 104 and 275 IU/L, respectively, and their levels were highest (797 and 671 IU/L, respectively) on day 3 (Fig. 5.). A pancreatic pseudocyst was developed during follow-up period and succesfully treated by percutaneous drainage.
DISCUSSION
Pancreatic injuries caused by trauma are rare but associated with significant morbidity and mortality. Heuer et al. [1] reported the results of pancreatic injury through the Trauma Register of the German Society of Trauma Surgery (TRDGU) (1993-2009). In this study mortality was 30.0% for grade IV pancreatic injury. Mohseni et al. [2] reported mortality of penetrating grade IV pancreatic injuries through trauma quality improvement (TQIP) databank analysis. In this study, mortality was 24.0% in the resection group and 27.1% in the non-resection group (p=0.68). However, there are reports that surgical management has better prognosis for grade IV pancreatic injuries confirmed by CT or surgery [3,4].
American Association for the Surgery of Trauma (AAST) defines grade IV pancreatic injury as proximal transection to the right of the superior mesenteric vein (SMV) or parenchymal injury involving the ampulla. However, there are rare reports of CT images matching the surgeries. Therefore, we report a case of complete transection of the pancreas to the right of the SMV after blunt injury with typical images including surgical findings.