CASE
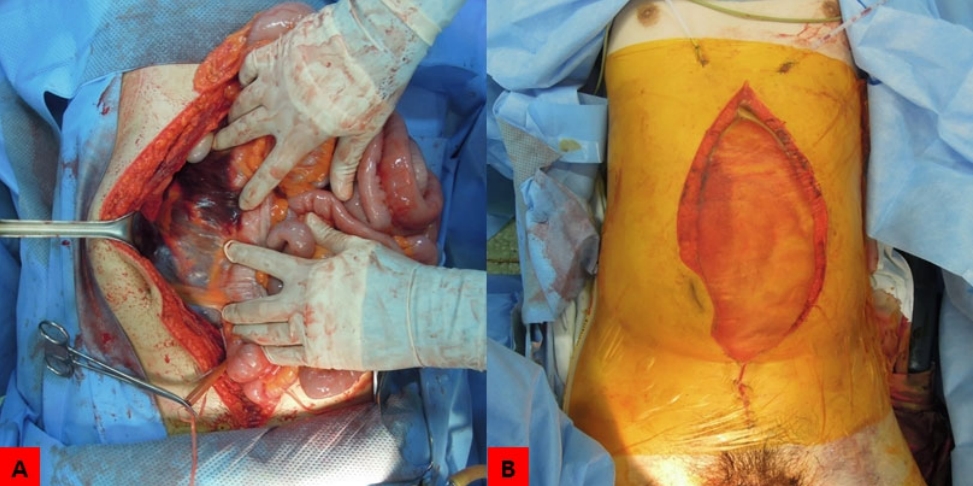
A 17-year-old male was referred to our emergency department from another hospital. He was struck by a dump truck while riding a bicycle. His initial vital signs were unstable: blood pressure, 90/50 mmHg; pulse rate, 122 beats/min; respiration rate, 27 breaths/min; body temperature, 34.9°C; and oxygen saturation, 99%. The pelvis was severely deformed by vertical shear (Fig. 1). Ligation of the left internal iliac artery and seromuscular repair of the sigmoid colon was performed in the emergency room. A large retroperitoneal hematoma and severe bowel edema were observed, and temporary abdominal closure was performed (Fig. 2). In addition, external fixation was performed on unstable pelvic fracture. The anal muscle was completely destroyed and the urethra could be directly touched by a finger. Post surgery, the patient was immediately moved to the interventional radiology room, where angioembolization was performed in the pelvis and left kidney to manage arterial bleeding (Fig. 3). Abdominal CT was performed, and it revealed a large retroperitoneal hematoma (Fig. 4). Thereafter, the patient was admitted to the intensive care unit. Abdominal wall closure was attempted on post operative day 4, but was challenging because of the large retroperitoneal hematoma and bowel edema. Therefore, abdominal wall closure was attempted using a 10×15-cm-sized acellular porcine dermal collagen (Permacol™; Covidien, New Haven, CT, USA). However, a sheet of Permacol™ was not enough to cover the abdominal wall defect. Therefore, the author performed abdominal wall repair using two 10×15-cm-sized PermacolTM Sheets longitudinally connected by a suture (Fig. 5). Additionally, the patient underwent a permanent loop ileostomy. The patient’s abdominal wall recovered well without complications (Fig. 6).
DISCUSSION
The treatment of complex abdominal wall defects in trauma patients is a challenging task for many surgeons. Recently, biosynthetic grafts such as human cadaveric dermis (AlloDerm™), dermal porcine (Permacol™ and Strattice™), and submucosal porcine (Surgisis™) have been used for this purpose [1]. Limura et al. [2] reported their experience in performing 56 complex abdominal wall reconstructions using Permacol™ in a single institute. In their study, mesh placement positions were intraperitoneal in 89%, retromuscular in 9%, and suprafascial in 1%. They reported that biomaterials used for definite repair of the complex abdominal wall can potentially reduce morbidity and improve reconstruction outcomes. Gentile et al. [1] reported satisfactory results without complications in a female patient after 12-month treatment with Permacol™ for infected abdomen with vast abdominal wall defect. Jimenez Gomez et al. [3] reported that large eventration occurred after the initial repair in a politraumatized male patient who developed important musculocutaneous avulsion and evisceration, and safe and effective results were obtained using Permacol™. They also reported that negative pressure therapy helped in wound closure. Treatment methods that do not use biological materials have also been reported. Lee et al. [4] reported a successful abdominal closure using the anterior rectus sheath turnover method and negative pressure therapy in a patient who underwent temporary abdominal closure after a damage control surgery. Several reports demonstrated that complex abdominal wall repairs were performed using various materials and methods. In the author’s knowledge, successful abdominal closure using two 10×15-cm-sized Permacol™ longitudinally connected by a suture has not yet been reported in the English literature.