CASE
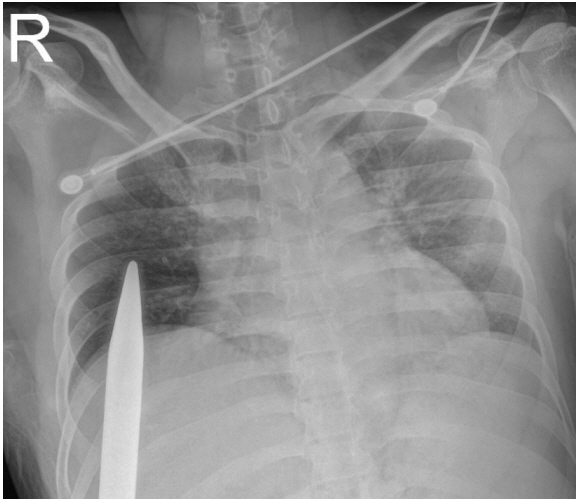
A 29-year-old male presented to our emergency department with a penetrating torso injury caused by a sharp and long steel bar. The patient slipped on a big straw pile and was struck on a protruding steel bar. The bar penetrated upward from the right flank to the middle portion of his right chest, and the rest of it was exposed toward his right foot. However, the patient only complained of pain at the right flank, and his vital signs were as follows: blood pressure, 120/70 mm Hg; pulse rate, 74 beats/min; respiratory rate, 26 breaths/min; body temperature, 37.2┬░C; and oxygen saturation, 98%. His arterial blood gas analysis revealed a pH of 7.38, pCO2 level of 38 mm Hg, pO2 level of 86.3 mmHg, and SaO2 level of 98%.
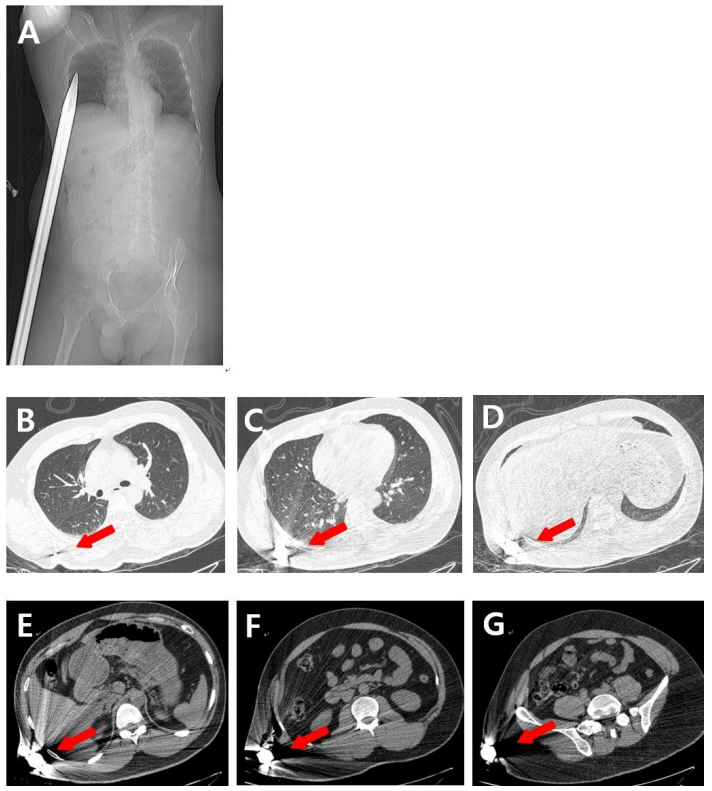
The patientŌĆÖs chest X-ray did not show any thoracic injuries, such as hemothorax or pneumothorax (Fig. 1.). Therefore, we next performed a thoracoabdominal computed tomography to examine any injuries in the thoracoabdominal organs (Fig. 2.). On confirming no injury, we next decided to perform an operation for the safe removal of the steel bar.
The patient was posed with left lateral decubitus under general anesthesia (Fig. 3.), which was carefully removed at first. Fortunately, it was removed without any resistance. The length of the removed steel bar was approximately 150 cm (Fig. 4.). The surgical drains were then inserted into the penetrating wound after a large amount of saline irrigation for the contaminated penetrating foreign body. The patient recovered and was discharged without any complications.
DISCUSSION
The severity of the injuries in penetrating trauma varies depending on the location and path of penetration. Penetrating injuries to the chest can involve superficial soft tissues of the chest wall, lungs and pleura, diaphragm, and mediastinum [1]. In addition, penetrating injuries to the abdomen can involve superficial soft tissues of the abdominal wall and solid organs, such as the liver, spleen, kidney, and hollow viscus.
Majority of the penetrating injuries need to be surgically treated. The selection of the appropriate surgical methods depends on the injury mechanics, trajectory, and hemodynamic status of the patients [2]. As in our case, although the wound was superficial, it was necessary to remove the embedded foreign material, clean it, and evaluate the precise status of the wound through a surgical approach. We created an incision to the existing wound to ensure that it was adequately cleaned in all trajectories. Moreover, the drain tubes were inserted in both the directions to obtain sufficient drainage.